
I was at my allergist’s office, exploring the anxiety/allergy connection. His nurse came in and asked me about my medications, what supplements I take, etc. all the routine questions. I told her about Lithium, Seroquel and then said “You know I have bipolar disorder?” She just looked at me, then asked “How have you done with it?”
How have I done with it? Well for someone with bipolar disorder, I’ve done remarkably well. I have two advanced degrees, a husband, a son, a beautiful home, even a blog.
But compared to someone “normal,” someone without any mental illnesses, I haven’t done well at all. I fight anxiety, depression, dark thoughts, emotions so intense they can be dangerous, I have no career and I worry constantly about my son. I worry he’s too much like me, ideally, he would only have an iota of me in him.
The latest thing is that my hair has started to fall out in bunches, which is a side effect of Lithium, possibly that’s what’s doing it. So now do I stop taking Lithium or lose all my hair? Also, I’ve been very clumsy lately, I have another concussion and broke my left pinky toe as a result of accidents. Clumsiness is also a side effect of Lithium. Again, do I keep having accidents or do I stop taking Lithium. Or lower the dose, which may not control my mood symptoms.
Everyday, something new, and not in a good way.
Feeling quite bad and overwhelmed. Bipolar or life? I suspect bipolar. Because I don’t always have this sick feeling in the pit of my stomach, this urge to cry, emotions sometimes so intense, I want to scream, to give up.
The diary of a manic depressive, welcome my friends, thank your lucky stars you’ll never have to live with this ghastly illness.
And yet, I won’t give up. These are the cards I’ve been dealt, I will play them with flourish and panache. And I think if I didn’t keep writing about it, no one might know what was going on inside my brain. So I keep giving myself away. But it is a release, it is therapeutic, to write. And if someone with cancer doesn’t have to hide their diagnosis and symptoms, why do mentally ill people have to be ashamed of theirs?
Oh well, I think I’m rambling now, so I’ll stop. I have no words of wisdom. I am no expert on anything. The only thing that keeps me going is my love for my son. And it is huge and it conquers all.
Posts
Disease Found in 99 Percent of Brains Donated by NFL Families
A game watched for entertainment, for players' feats of amazing athletic prowess! And in 99% of players' brains examined, there was evidence of chronic traumatic encephalopathy (CTE.)
The article below.
http://www.smithsonianmag.com/smart-news/cte-found-99-percent-brains-donated-nfl-families-180964202/?utm_source=facebook.com&utm_medium=socialmedia
The degenerative brain disease develops after repeated concussions or blows to the head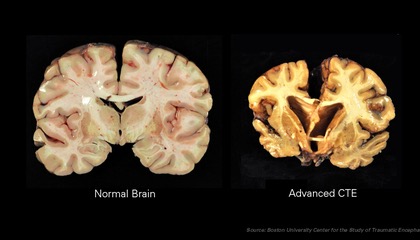
The degenerative disease, chronic traumatic encephalopathy or CTE, is common in football players, boxers, veterans and others exposed to head trauma. (Wikimedia Commons)
By Jason Daley
SMITHSONIAN.COM
JULY 25, 2017 4:07PM
311002159
Over the last decade, one of the biggest stories in sports has been the mounting evidence of chronic traumatic encephalopathy, or CTE, in football players. The degenerative brain disease develops after repeated blows to the head, and a new study finds a strong link between playing football and CTE. As Daniella Emanuel at CNN reports, the brains of 110 out of 111 NFL players that were donated to the researchers showed signs of the disease.
The study, published this week in the journal JAMA, was based on autopsies of 202 deceased football players including those who did not play beyond the high school and college level. As Emanuel reports, in addition to the NFL players, the disease was found in 48 out of 53 college players and 3 of the 14 high school players.
The brains examined for the study came from subjects that ranged in age from 23 to 89 and from every position on the football field, from punters to linebackers, Joe Ward, Josh Williams and Sam Manchester report for The New York Times. In the brains examined, the largest number of CTE cases were found in linemen, running backs and defensive backs. Eighty-six percent of the professional players in the study had severe cases of the disease as did 56 percent of the college players.
“There's no question that there's a problem in football. That people who play football are at risk for this disease,” Ann McKee, director of Boston University's CTE Center and coauthor of the study tells Emanuel. “And we urgently need to find answers for not just football players, but veterans and other individuals exposed to head trauma.”
According to the Concussion Legacy Foundation, a CTE advocacy and research group, the disease occurs when clumps of a protein called Tau, which destroy brain cells, develop after repeated head trauma. The disease usually progresses over time, causing memory loss and confusion, impaired judgment and eventually dementia. The disease usually impacts a sufferer’s mood and behavior in their 20s and 30s, progressing to cognitive impairments in their 40s and 50s. Besides football players, boxers and combat veterans are also at risk for CTE.
It's important to keep in mind that the samples in the study are not randomly selected. As McKee tells The New York Times, the study sample suffers from "tremendous" bias since most of the brains studied were donated by families that suspected their loved one suffered from CTE, which currently can only be diagnosed post-mortem. That bias makes it difficult to figure out what percentage of current football players may develop CTE.
Even so, the results strengthen the link between football and CTE and highlights what researchers don’t know. “There are many questions that remain unanswered,” McKee tells ESPN.com. "How common is this? How many years of football is too many? What is the genetic risk? Some players do not have evidence of this disease despite long playing years.” She also notes there is a possibility that drug use, steroids, alcohol abuse and diet could also contribute to the onset and progression disease.
As ESPN.com reports, the NFL denied the links between football and CTE for years, but in 2015 the league settled a class action lawsuit brought by former players. The league will pay up to $1 billion in medical costs for 20,000 current and former players who suffered concussions and now experience potential CTE-related problems, according to NPR. In 2016, the League made it’s first public acknowledgement that there is likely a connection between playing football and CTE. And as Emanuel reports, in recent years the NFL has changed protocols surrounding concussions and discourages full-tackle football for children.
In a statement, the NFL calls the study valuable and says it is committed to supporting continued scientific research into CTE, reports Jessica Glenza at The Guardian. “My hope is we’ll stop arguing about whether or not this is a problem, or whether or not it needs to be addressed,” McKee tells Glenza. “We need to take our heads out of the sand. It’s not going away because we want it to.”
Ruins Speak
http://www.lulu.com/shop/wajahat-fatima/ruins-speak/paperback/product-23268503.html
This is the link to my aunt's amazing, poetic, autobiographical book in Urdu, called "Ruins Speak". I'm working on translating it into English.
Can Cardio Exercise Aid in Concussion Recovery?
According to John Leddy, the director of the University at Buffalo’s Concussion Management Clinic, controlled cardio exercise is good for recovering from concussions.
http://www.athleticbusiness.com/high-school/can-cardio-exercise-aid-in-concussion-recovery.html
Long considered a forbidden activity for individuals with concussions, cardiovascular exercise is slowly becoming recognized as a recovery tool.

For that, you can thank physician John Leddy. As the director of the University at Buffalo’s Concussion Management Clinic, where he also is an associate professor of orthopedics, family medicine and rehabilitation sciences, Leddy for the past five years has conducted research suggesting that supervised workouts on treadmills, stationary bikes, ellipticals or stair-steppers – performed for as little as 10 minutes at 80 percent of a patient’s target heart rate – can help in the recovery process. He also claims a cardio workout provides a clearer indication than cognitive testing of when an athlete is ready to return to play.
“Everybody thought that doing something like this would make people worse, not better,” says Leddy. “But it does make them better, because it’s controlled. Fifty years ago, when doctors started doing stress tests on people with cardiac disease, people thought that would give them heart attacks. But the fact is, stress tests don’t do that. And now those tests are done as a matter of routine.”
If Leddy has his way, his exercise protocol for concussion patients will become routine, too, and he points to rehab clinics around the country that have already adopted some of his ideas. “It’s okay, at some point, for people with concussions to begin exercising again, as long as they’ve seen a doctor and had testing done under medical supervision,” he says. “As this catches on, you might see people in health clubs or fitness facilities who are actually doing this program and trying to recover from concussion symptoms.”
For now, though, UB appears to be the only facility undertaking outcome-based studies in this area. That’s why, in September, the university was among the 15 organizations to receive a sports-related medical research grant from NFL Charities to take the next step. Using the $100,000 grant, Leddy and Barry Willer, a UB professor of psychiatry and rehabilitation services, will spend this year assessing the fitness levels of student-athletes from several area colleges, plus members of the Buffalo Bills and the Buffalo Sabres, within hours of being diagnosed with a concussion.
“We haven’t done early assessments like that yet,” Leddy says. “But we think the physiology is different right after a concussion versus when someone is recovered. We want to see if the treadmill test is a good way to find out if there is a change in cerebral blood flow when they are symptomatic during exercise versus when they are not.”
The 18-month study began in earnest in January and will include as many as 30 injured athletes and 30 healthy control subjects. The results, as Bills’ executive vice president for strategic planning Mary Owens told UB Reporter, the University at Buffalo’s online staff newspaper, “will benefit athletes at all levels.”
“Replacing the conventional wisdom of long-term rest with a graduated exercise program may improve recovery in those with lingering concussion problems,” acknowledges Stanley Herring, a member of the NFL Head, Neck and Spine Committee and a team physician with the Seattle Seahawks and the MLB’s Seattle Mariners. “A study like this is important because it explores a potential treatment for athletes with persistent concussion symptoms.”
Persistent concussion symptoms are those that linger for more than two or three weeks. Though they affect only a small percentage of concussed athletes, they are what got Leddy (also a doctor for UB athletic teams) thinking differently in the first place. “Why should these athletes be sitting around doing nothing? Why can’t they do something, something that’s controlled and safe?” he asks. “Physical rest beyond three weeks is detrimental.”
So he asked student-athletes with lasting concussion symptoms to hop on a treadmill while he monitored such vitals as blood pressure and heart rate. Patients would exercise to the point where their symptoms – such as dizziness and headaches – increased, and Leddy would then stop the machine and establish 80 percent of whatever the patient’s heart rate was at that moment as the new target heart rate for daily 20-minute workouts. After all, he reasoned, the individual had already proved he or she could exercise at that level without becoming symptomatic. For high-performance athletes, the target heart rate can be increased to 90 percent, while deconditioned individuals who suffer a concussion from an accident or other non-athletic incident may be prescribed a maximum of 10 or 15 minutes of exercise at 80 percent.
Leddy and Willer, who chose 80 percent arbitrarily, based their early research on similar studies (involving concussed rats) conducted at UCLA in the early 2000s. “What those studies told us was that maybe exercise isn’t so bad; it’s the timing that is important,” Leddy says. “It’s not just telling people to go out and do whatever they want. It’s quantifying what they can do and building a rehab program around that information. Now, we tell patients to go to a gym and use a piece of equipment they like that doesn’t involve a lot of bouncing and movement of the head. We want them to get an aerobic workout.”
Leddy and his research colleagues also want to ensure their athletes are ready – really ready – to return to play. Cognitive baseline testing, they say, might not be the answer.
“Most people view concussion as a cognitive problem,” Leddy says. “We view it as a physiological problem that has cognitive consequences. Therefore, what the NFL study may show is that doing a physiological stress, like exercise, is actually a better way to determine if someone has recovered than the cognitive testing that all sports teams use. We wanted something that is more representative of what athletes do on the field, and that is get their heart rate and blood pressure up. The real test for football players is to see if they suffer from any symptoms when they go back to hitting.”
To that end, an obstacle course could be designed in a clinical setting involving participants running in a figure-eight pattern and then colliding with a heavy punching bag, as well as participating in a cardio test. “What I’m hoping is that someday, instead of using a computer test to determine if Michael Vick has recovered from a concussion, they’ll put him on a treadmill. Or maybe they’ll do both,” Leddy says.
Still, some skeptics will need more convincing. Isn’t it risky, they might ask, to take concussed patients to the brink of dangerous symptoms? “We’ve thought about that, for sure,” Leddy concedes. “Do that to people, and they will get worse temporarily – for several minutes or several hours – but it doesn’t last. At least with this, they’re doing something active, and what happens right away is their reactive depression goes away. So if they can exercise and they have a goal, they automatically feel better. They make progress. They see an end point. The exercise is doing something physiologically, but also psychologically, to help them.”
Scientists Have Reversed Brain Damage in a 2-Year-Old Girl Who Drowned in a Swimming Pool
This is incredible, a little girl drowned. She was in the water for 15 minutes before her mother found her and started administering CPR. She had no heartbeat for 2 hours afterwards! And she “showed deep grey matter injury and cerebral atrophy with grey and white matter loss after the incident.”
After treatment with Oxygen and Hyperbaric Oxygen, the brain damage has been reversed, she is walking, smiling, she is herself again!
This is truly amazing! Oxygen! Also considering her young age and the ability of her brain to also heal on its own, I believe she will be as right as rain!
Amazing, and miraculous! Oxygen!
She was in the water for 15 minutes.
Researchers in the US have reported what they believe is a first-of-its-kind reversal of brain damage, after treating a drowned and resuscitated toddler with a combination of oxygen therapies.
The little girl, whose heart didn’t beat on her own for 2 hours after drowning, showed deep grey matter injury and cerebral atrophy with grey and white matter loss after the incident, and could no longer speak, walk, or respond to voices – but would uncontrollably squirm around and shake her head.
Amazingly, thanks to a course of oxygen treatments – including hyperbaric oxygen therapy (HBOT) – administered by a team from LSU Health New Orleans and the University of North Dakota, doctors were able to significantly reverse the brain damage experienced by the toddler.
“The startling regrowth of tissue in this case occurred because we were able to intervene early in a growing child, before long-term tissue degeneration,” says hyperbaric specialist Paul Harch from the LSU Health New Orleans School of Medicine.
The drowning occurred in February of last year, when two-year-old Eden Carlson slipped through a baby gate while her mother took a shower, then made it past a heavy door, before eventually falling into the family swimming pool.
She was in the water for 15 minutes before being discovered and had experienced cardiac arrest, and while her mother immediately began CPR, Eden wasn’t successfully resuscitated for 2 hours, being eventually revived by doctors at Washington Regional Medical Centre in Fayetteville, Arkansas.
After receiving critical care in hospital for 48 days, the little girl was discharged, but due to the extent of her brain injuries and their physical side effects, Harch proposed treatment with oxygen therapies in an attempt to “wake up” Eden’s damaged brain.
Hyperbaric oxygen therapy works by administering oxygen to a patient at an ambient pressure higher than atmospheric pressure, through the use of a sealed, pressurised chamber.
By doing this, the amount of oxygen in a patient’s blood supply is increased, which can restore normal levels of blood gases and repair damaged tissue.
In this case, Eden wasn’t located close enough to a hyperbaric oxygen therapy chamber, so the team began a bridging course of normobaric oxygen treatments – delivered at sea level pressure – at fifty-five days after the drowning.
The treatments, given for 45 minutes twice a day through a nasal cannula, saw Eden recover alertness and reduced her squirming, giving her back increased movement of her arms and hands.
She also regained part of her ability to eat orally, and could speak short sequences – and laugh.
About three weeks later, the researchers moved Eden and family to New Orleans, where she began a round of new treatments in a hyperbaric chamber.
After just 10 sessions, Eden’s mother observed that the toddler was back to “near normal, except for gross motor function”, and so the little girl began physical therapy in addition to the hyperbaric treatment.
Once 39 hyperbaric sessions were completed, Eden’s walking had improved, and her speech level was assessed to be now greater than it was at the time of the drowning. She demonstrated improvements on all neurological abnormality tests, and showed near normal motor function and cognition.
At the conclusion of the treatment, some 162 days after she drowned, MRI scans revealed that Eden still bore a mild residual injury to her brain, but had experienced a near-complete reversal of cortical and white matter atrophy.
The team studying her recovery say that to their knowledge, this kind of reversal is “unreported with any therapy”.
And while they don’t fully understand the exact breakdown of this amazing revival in Eden’s fortunes, it’s clear that normobaric and hyperbaric oxygen treatments combined to reduce inflammation and promote brain cell survival.
“Although it’s impossible to conclude from this single case if the sequential application of normobaric oxygen then HBOT would be more effective than HBOT alone, in the absence of HBOT therapy, short duration, repetitive normobaric oxygen therapy may be an option until HBOT is available,” Harch says.
“Such low-risk medical treatment may have a profound effect on recovery of function in similar patients who are neurologically devastated by drowning.”
The findings are reported in Medical Gas Research.
Underlying molecular mechanism of bipolar disorder revealed
 This is an interesting article! Bipolar disorder has always been thought to be a genetic disorder, that is due to mutations in genes. One of the reasons bring it is inherited and runs in families. However, here the authors make a case for it not being genetic but physiological in nature. I’ve put the most important passage in the article in quotes below. If you’d love to read the whole article, there’s, as always, a link below too. CRMP2 is a protein that is involved in neural networking, i.e in arranging neurons from soma to axon and making networks between neurons. In bipolar disorder, the activity of this protein is low. When Lithium is given to Lithium responsive neurons, the activity of CRMP2 is brought back up to normal, thereby correcting the underlying cause of the disorder. That’s what the authors say. Just have to wait and see if this is truly the underlying cause of bipolar disorder.
This is an interesting article! Bipolar disorder has always been thought to be a genetic disorder, that is due to mutations in genes. One of the reasons bring it is inherited and runs in families. However, here the authors make a case for it not being genetic but physiological in nature. I’ve put the most important passage in the article in quotes below. If you’d love to read the whole article, there’s, as always, a link below too. CRMP2 is a protein that is involved in neural networking, i.e in arranging neurons from soma to axon and making networks between neurons. In bipolar disorder, the activity of this protein is low. When Lithium is given to Lithium responsive neurons, the activity of CRMP2 is brought back up to normal, thereby correcting the underlying cause of the disorder. That’s what the authors say. Just have to wait and see if this is truly the underlying cause of bipolar disorder.
https://m.medicalxpress.com/news/2017-05-underlying-molecular-mechanism-bipolar-disorder.html
“In hiPS cells created from lithium-responsive and non-responsive patients, researchers observed a physiological difference in the regulation of CRMP2, which rendered the protein to be in a much more inactive state in responsive patients. However, the research showed that when lithium was administered to these cells, their regulatory mechanisms were corrected, restoring normal activity of CRMP2 and correcting the underlying cause of their disorder. Thus, the study demonstrated that bipolar disorder can be rooted in physiological—not necessarily genetic—mechanisms. The insights derived from the hiPS cells were validated in actual brain specimens from patients with bipolar disorder (on and off lithium), in animal models, and in the actions of living neurons.”
Twisted
 Tomorrow I go home Tomorrow I start worrying again. Tomorrow anxiety will hijack my brain again.
Tomorrow I go home Tomorrow I start worrying again. Tomorrow anxiety will hijack my brain again.
It will take me through twisted, tortuous roads, it will show me in sickening, horrifying detail what can go wrong and convince me that it all will go wrong.
It will hijack my brain and my mind for half the day. Yes half the day. For the rest, it will grant me respite. I will be free to be me for the second half of the day. I will make the most of it. I will make plans of how to defeat anxiety tomorrow. “Get up, don’t listen to your thoughts, get out and go for a brisk walk. Set your coffee out on your bedside table and drink it the moment you open your eyes, watch something funny on YouTube, etc. etc…”
I won’t let it beat me. It’s not real. And then the thought sneaks in: Isn’t it real? Aren’t all those things possible? God if anyone is a master at playing mind games, head games, it is anxiety. And I hate it that it’s using my head as the playing field.
Tomorrow I will go home and I will be the unwilling star player in this god awful, sick, twisted game. All the while, I’d rather be dancing. 💃🏻💃🏻💃🏻💃🏻
Feel Too Much
 Sometimes I just want to break down and cry
Sometimes I just want to break down and cry
At the exquisite beauty of life
At the hideousness of it
At the warmth and tenderness
At the frigid, iciness
At the loving arms enveloping me
At the cruel feet kicking the life out of me
At my terrifying, heartbreaking love for my precious child
At the fear and terror that everything will go wrong
At the family gatherings with love, care, and compassion. Loving togetherness
And the aching goodbyes, the pangs of missing each other, “Oh we were all together just yesterday!”
Feel and feel and feel too much
My heart cries out at your tender touch
Time to up the Lithium? Yes, if it gets any deeper than this.
Beauty and feelings mean nothing to me if I’m in the hospital in a freaking manic phase.
Helping myself
 Wow! Sometimes you do something only in the spirit of helping someone, and it totally comes back to bite you in your derrière. You don’t have to do this thing, you are under no obligation to do it. But for some reason you feel someone is asking for your help without using the exact words, so you actually try to help. My advice was actually to read “The Power of Now” by Eckhart Tolle. Also it was about the effects of L-Dopa when people first start taking it for early onset Parkinson’s disease. How that advice could be taken wrongly and twisted to make me feel like I’d done something wrong is quite puzzling and quite beyond me.
Wow! Sometimes you do something only in the spirit of helping someone, and it totally comes back to bite you in your derrière. You don’t have to do this thing, you are under no obligation to do it. But for some reason you feel someone is asking for your help without using the exact words, so you actually try to help. My advice was actually to read “The Power of Now” by Eckhart Tolle. Also it was about the effects of L-Dopa when people first start taking it for early onset Parkinson’s disease. How that advice could be taken wrongly and twisted to make me feel like I’d done something wrong is quite puzzling and quite beyond me.
Do I stop helping people? If someone reaches out to me either in words or actions, do I just ignore them to avoid the backlash? Yes. For a bit. Until I understand how trying to help someone is wrong. I’m going to stop. For self preservation. For my own peace of mind and for the peace in my life. I’m going to put myself first. And not go out on a limb to help anyone else.
I have always been helpful and selfless. But this incident is teaching me how to be more selfish and less selfless, so that I cannot be turned into the scapegoat into which I have frequently been turned. My entire life. I think I needed that lesson.
Overcoming the “8 Reasons Why People Don’t Get Treatment for Mental Illness” by Dr. David Susman.
Pretty great article for anyone struggling to accept they have a mental illness. So many reasons not to accept that we have these wretched illnesses. Dr. Susman offers alternative ways of looking at things, more helpful and constructive ways. Would be a great read for relatives of those struggling with mental illness as well.
Me, after my first depression, at which point I had no idea what the hell happened to me, but after that, I realized and accepted that I suffered from a mental illness. My first manic phase when I was Alice in Wonderland, and what a wonderland it was, well it was quite difficult to disavow my illness. After that first manic phase, I of course had to accept that I had bipolar 1. And though I’ve lost my baby brother to this illness, 31 years after my diagnosis, I’m still here.
As per the author’s request, I am removing the text of the article here, please just click on the link to read it 🙂
